This Bipolar Blog post is a guest post coming in from Julia Lukacs, M.Sc. You may recall how last year, Julia shared a post about a study looking at how people’s reactions to the COVID-19 pandemic relate to risk-taking behaviour. In this post, she shares findings from the study about how that way we think about a risk influences how we act.
Dr. Perez Algorta and I have been focusing our research on how risk-taking plays a role in our lives.
A year ago, we appealed for your help in our survey of risk-taking during the recent pandemic. Although much has changed since that time, many areas are currently entering a third wave of the pandemic and a number of concerns remain similar. In this article, we are eager to share what we have learned with you.
Whether or not we take a risk is partially determined by our understanding of risk (risk perception). These perceptions are largely influenced by past experiences and knowledge. Understandably, immediate, visible threats get more of our attention than those risks that are less visible. For example, we are more likely to interpret walking down a dimly lit street as risky than adding salt to every meal. As a result, diffuse problems, such as global warming and epidemics are not always readily conceptualized as risky. This is particularly more likely to happen when these problems begin.

During the COVID-19 pandemic, everyday behaviors that were previously safe, such as grocery shopping or seeing a friend, became risky. The high speed of the virus transmission, and the typically benign nature of the behaviors that we all had to change, made this a pertinent moment to explore risk perceptions, and risk taking behaviors.
We ultimately hoped to better understand how individual perceptions of risk changed in this short time.
What’s behind risk-taking behavior?
We used Fuzzy-Trace Theory, a theory of risk taking, to understand behaviors and beliefs. Fuzzy Trace Theory categorizes our memories and perceptions into two groups:
- Gist based memories and decision-making processes, that focus on the bottom line idea behind a given memory (e.g. “Smoking is bad for your health and isn’t worth the risk”), and
- Verbatim based decision-making processes, that are concrete and more detail-focused (e.g.. “Smoking is related to 80% of lung cancer deaths.”)
According to the theory, gist thinking leads to less risk taking than verbatim thinking, even though both types of thought are related to risk. We expected that individuals would decrease their high-risk behaviors (such as, group activities) and increase their low-risk behaviors (such as distance communication) at the beginning of the COVID-19 pandemic if they showed more gist thinking than verbatim thinking.
What did we find?
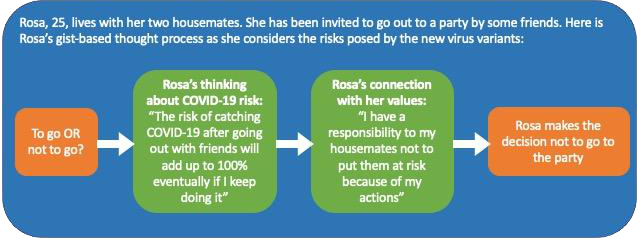
We also saw that gist thinking could be further nuanced: categorical views on risk, although still gist-based e.g.. “even low risks adds up to 100% if you keep going outside or in public enough”) seemed to impact risk taking through larger value-based gist statements ( e.g. “I have a responsibility to the people I live with to not put them at risk”). These categorical views did not seem to impact risk on their own; it seems the core, value-based gist was needed to change risk behaviors. Overall, this means that the value attached to gist may hold importance for reducing risk (see example vignette in diagram below).
The challenge of reducing risky behaviors is that, ideally, motivation should come from the individual and no one should be forced to make decisions or change their behavior.
Our study shows that among those individuals who are already attentive to messages about risk, a gist-based, broad, analytical perspective may lead to lower-risk behaviors, and Fuzzy Trace Theory may be a valuable way of thinking about these issues and informing strategies to reduce negative outcomes associated with risk taking behaviors (e.g. death).
Indeed, our group has found similar results when looking at sexual risk-taking behaviors in a survey of individuals with bipolar disorder diagnoses. A recent qualitative study showed that risk seems to play an important role in the lives of individuals with BD diagnoses, and a thorough understanding of risk and how it functions may be important in prevention and treatment.
The path ahead
Of course, there is still much work to be done. These studies are voluntary, survey-based studies. People who want to answer questions about their behaviors related to a pandemic so that researchers can then answer questions about society are most likely: (a) people who are concerned about the pandemic and (b) interested in scientific research in general. Therefore, they may be more likely to be attentive to public health guidelines.
In this study, the sample also identified as overwhelmingly female and the average age was around 40. Women are less likely to take risks (more risk-averse), and the older someone is, the less likely they are to take risks. We may see something different in a younger or more diverse sample. We see similar patterns in the demographic characteristics of people participating in our studies focused on people with a BD diagnosis. For example, the level of education in those samples is 60% with an undergraduate degree or higher, while average level of individuals with an undergraduate degree and with a diagnosis of BD, according to BD case registries, is 30%.
It is possible that part of the solution to these issues of representativeness (validity) in research requires new creative strategies driven by participatory research. Participatory research is the effort to transfer some of the power over research (currently overwhelmingly in the hands of researchers and financing bodies) towards community members or organizations.
In 1961, the famous psychologist and researcher Carl Rogers wrote, “it is the client who knows what hurts, what directions to go, what problems are crucial, what experiences have been deeply buried.” He revolutionized psychotherapy by placing the client first and encouraging therapists to talk less and listen more. Research has begun to actively consider how we can place the participant first, but we are far from mastering participatory practices. Today, organizations like CREST-BD contribute greatly to participatory research, through outreach and initiatives like this blog. We sincerely hope that more work like this will continue in the future.

Given this, our results in this study are promising. Fuzzy Trace Theory may be a useful way of thinking about risk-taking in public health initiatives. Next steps for work in this area might include further study in different groups, and the development of preventive and treatment modules that can be adopted in various therapeutic settings.
Ultimately, we are grateful to individuals like you, who help us find responses to the questions we are asking. Now it’s our turn to ask again- what do you think? If you were invited to participate in a similar project, what would motivate you to partake? If you were to participate in a treatment, what conversations about risk would you like to have? How have you seen these concepts in action in your life? Let us know in the comments, or by sending us an email! We look forward to hearing from you.
Contact Us
Guillermo Perez-Algorta, Ph.D. – g.perezalgorta@lancaster.ac.uk
Julia N. Lukacs, M.Sc. – julia_lukacs@sfu.ca


Leave a Reply